

Estimated reading time: 7 minutes
Most people need corrective exercise — they just don’t realize it. This type of programming is not reserved for the injured or the symptomatic. If your body compensates when it moves, it applies to you.
At Body360 Fit, we assess every client before any training begins to find asymmetries and dysfunction so we can create the right training plan for you.
Key Highlights
- Feeling fine doesn’t mean moving well — problems build quietly before anything hurts
- Desk workers over 35 are among the highest-risk groups due to years of accumulated sitting patterns
- High-volume trainers repeat flawed mechanics under load — the damage compounds with every session
- Recurring discomfort almost always traces back to a movement problem that no one has looked for
- Post-rehab clients need to correct what caused the injury, not just recover from it
- Every program at Body360 Fit starts with a functional movement screen — results drive everything
Corrective Exercise Is Not Just for People in Pain
Pain is a late signal. By the time pain shows up, the dysfunction driving it has usually been present for months or years. Most people who need corrective exercise feel completely fine — they train, they function, they have no obvious symptoms. But underneath, the body is compensating quietly, and those compensations accumulate.
Catching these patterns early is always easier than fixing them after the fact — and the reason we screen before we train.
Desk Workers, Postural Issues, and Professionals Over 35
This is the group we work with most at Body360 Fit. Hours at a desk, looking at screens, doing the same motions every day — the body adapts to those demands. A posture assessment reveals the postural issues that have built up, and for most professionals, what shows up on screen is more than they expected.
- Rounded shoulders — the chest pulls the shoulders forward, which limits pressing and overhead work
- Anterior pelvic tilt — overactive hip flexors and weak glutes, which contribute to low back pain
- Forward head posture — the deep neck muscles stop working, and the cervical spine absorbs the load
- Thoracic restriction — the mid-back stiffens from sustained sitting, so the low back compensates
- Hip flexor tightness — limits hip extension and directly affects squatting, walking, and glute strength
After 35, the body tolerates these patterns less. What once felt manageable starts to show up as stiffness, restriction, or pain — and training on top of it only accelerates the process.
Athletes and High-Volume Trainers
Being fit doesn’t mean moving well. High training volume doesn’t fix bad mechanics — it loads them harder and faster. The same flawed pattern repeated thousands of times builds structural stress with every rep, often for years before anything hurts.
- Runners — hip drop, knee cave, and overstriding load the IT band, knee, and low back with every stride
- Cyclists — a sustained forward lean tilts the pelvis and switches the glutes off entirely
- Swimmers — poor shoulder mechanics under high volume gradually break down the rotator cuff
- Racquet players — one-sided loading builds shoulder and rotation imbalances over time
- Weightlifters — tight mid-back and hips compromise squats, deadlifts, and anything overhead
For athletes, corrective work is about moving better under load — more output, less breakdown, and a longer training life.
Corrective Exercise for Chronic Pain and Post-Rehabilitation Clients
If you’re in active pain, the first call is to your doctor or physical therapist. We don’t start corrective work until you receive medical clearance
Once cleared, the work begins. Rehab addresses the injury — corrective exercise addresses the cause. Too many people finish their rehabilitation exercises and return to the same mechanics that created the problem, and then wonder why it comes back. Active individuals and anyone struggling with recurring issues after rest, stretching, or rehab almost always have a compensation pattern that no one has identified.
Alleviating the symptom at the site is not the goal — finding what’s driving it is. We help strengthen weakened muscles, retrain the patterns that failed under load, and eliminate pain triggers for good. At Body360 Fit, we coordinate with therapy teams directly so our work picks up exactly where treatment ends.
How an Exercise Specialist Identifies the Problem
A movement screen is what separates a corrective program from regular training. A functional assessment — including movement compensations, basic movement patterns, and rotary stability — reveals where the body compensates. Foundational patterns like the deep squat, inline lunge, and hurdle step reveal limitations in mobility, stability, and control. Those findings drive the corrective plan.
The screen goes beyond what a posture photo or pain questionnaire reveals. Breakdowns that aren’t visible at rest show up under load — single-leg stability, hip hinge mechanics, rotary control, overhead patterns. We build the corrective plan around exactly those patterns.
Muscle Imbalances, Asymmetries in Strength, and Motor Control
These are the most common findings from a corrective screen — and what we do to remedy each one.
| Issue | How We Find It | What We Do | Result |
|---|---|---|---|
| Poor motor control | Functional movement tests | Muscle activation, pattern retraining | Better efficiency under load |
| Asymmetries in strength | Side-to-side load testing, single-leg assessment | Targeted functional strength work | Balanced strength, better stability |
| Poor movement mechanics | Technique and load observation | Pattern retraining, progressive loading | Functional strength, fewer injuries |
| Postural problems | Posture and gait analysis | Corrective sequence, postural work | Less pain, better alignment |
Common Conditions and What Corrective Work Does
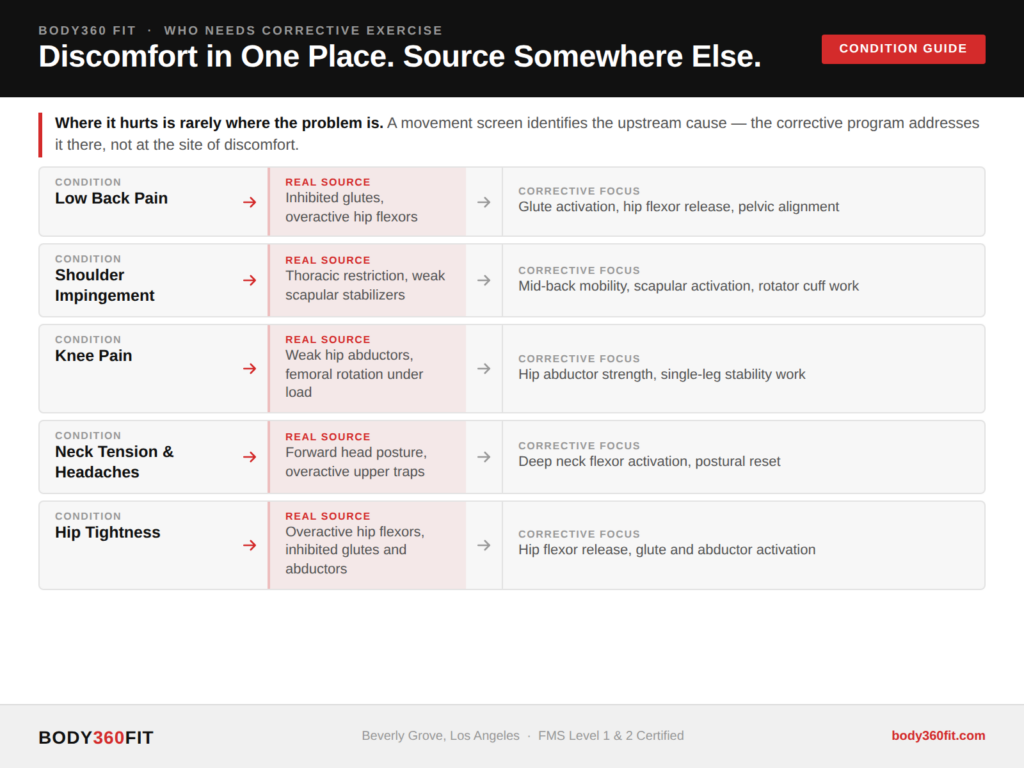
Pain in one area of the body usually means the source is the joint above or below. A sore knee often starts at the hip. A painful shoulder often starts in the mid-back.
Generic training programs miss this because they treat the diagnosis rather than the screen findings — and two people with identical symptoms often need completely different approaches.
- Low back pain — usually a hip and glute problem, not a spine problem
- Shoulder impingement — typically a mid-back and shoulder blade issue, not a shoulder issue
- Knee pain — often originates at the hip, not the knee
- Neck tension and headaches — forward head posture loading the neck throughout the day
- Hip tightness — overactive hip flexors and weak glutes, limiting all lower body function
We see corrective exercise work across desk workers, post-rehab clients, competitive trainers, and people who have never trained.
What the Corrective Exercises and Plan Look Like
Every plan starts with a functional movement screen. From there, a corrective specialist builds a sequence specific to what the findings showed — not a template, not a generic protocol. The exercises, order, frequency, and progression are all specific to you.
Phase One
Phase One reduces excessive muscle tone and prepares the body to move.
We use foam rolling and targeted drills to down-regulate overactive tissue, followed by movement prep to engage the nervous system and restore motor control and coordination.
- Foam rolling drills — reduce tone in overactive muscles and improve tissue quality
- Targeted corrective work — restore balance where control has been lost
- Movement prep — activate the nervous system through controlled, dynamic movement
Phase Two
Phase two integrates functional strength into real movement under load.
Strength improves, output increases, and the body stops working against itself. For post-rehab clients, this is where confidence returns and your body begins to move the way it’s supposed to.
This is the foundation on which everything else is built.
If movement isn’t correct here, strength work reinforces the compensation. The body will always work around the weak link — and that becomes the next problem.
When movement is corrected first, strength builds the right pattern — not the workaround.
Most people feel a real shift within four to six weeks. For many clients, a deeper understanding of what corrective exercise is provides the why behind their program — and the confidence to keep following it.
The Bottom Line
Whether you sit at a desk, train hard, deal with recurring discomfort, or are coming back from injury, you are a candidate. The question isn’t whether corrective exercise applies to you. It’s how much discomfort you’re willing to let it continue.
Most people who come to Body360 Fit are surprised by what our fitness assessment reveals. Not because the findings are alarming — but because patterns they’ve carried for years, compensations they assumed were just how their body works, turn out to be entirely correctable.
— Christian Graham
Founder, Body360 Fit

")

![Full Body Kettlebell Workout [PDF] | Body360 Fit](https://body360fit.com/wp-content/uploads/2021/01/Full-Body-Kettlebell-Workout-PDF.png)







